Free Preparation Discussions
ARDMS AE-Adult-Echocardiography Exam Questions
- Topic 1: Anatomy and Physiology: This section of the exam measures skills of adult echocardiography technicians and covers knowledge and abilities related to normal cardiac anatomy and physiology. It includes assessing great vessels like the aorta and pulmonary arteries, recognizing anatomic variants of the heart, and evaluating cardiac chambers, pericardium, valve structures, and vessels of arterial and venous return. Candidates must document normal systolic and diastolic function, normal valve function and measurements, the phases of the cardiac cycle, normal Doppler changes with respiration, and appearance of arterial and venous waveforms. This also involves assessing the normal hemodynamic response to stress testing and maneuvers such as Valsalva, respiratory, handgrip, and postural changes.
- Topic 2: Pathology: This section of the exam measures skills of adult echocardiography technicians and focuses on identifying and evaluating abnormal physiology and perfusion and postoperative conditions. It includes assessment of ventricular aneurysms, aortic and valve abnormalities, arrhythmias, cardiac masses, diastolic dysfunction, endocarditis, ischemic diseases, cardiomyopathies, congenital anomalies, and postoperative valve repair or replacement and intracardiac devices. Candidates must demonstrate ability to recognize abnormal Doppler signals, EKG changes, wall motion abnormalities, and a wide range of cardiac pathologies including pulmonary hypertension and septal defects.
- Topic 3: Clinical Care and Safety: This section of the exam measures skills of adult echocardiography technicians in applying clinical care principles and safety protocols. It includes evaluating patient history and external data, preparing patients including fasting state and intravenous line management, proper patient positioning, EKG lead placement, blood pressure measurement, and ergonomic techniques. Candidates are expected to identify critical echocardiographic findings, know contraindications for procedures, and be able to respond and manage medical emergencies that may arise during echocardiographic exams.
- Topic 4: Measurement Techniques, Maneuvers, and Sonographic Views: This section of the exam measures skills of adult echocardiography technicians in performing accurate cardiac measurements, conducting provocative maneuvers, and obtaining optimized sonographic imaging views. It involves applying 2D, 3D, M-mode, and Doppler techniques to measure heart valves, chambers, and vessels, including the aortic valve, mitral valve, left and right ventricles, atria, pulmonary artery, and shunt ratios. Candidates must instruct patients in maneuvers such as Valsalva, cough, sniff, and squat. They should also be proficient in acquiring standard echocardiographic views including apical, parasternal, subcostal, and suprasternal notch views.
- Topic 5: Instrumentation, Optimization, and Contrast: This section of the exam measures skills of adult echocardiography technicians related to use and optimization of ultrasound instrumentation and the application of contrast agents. Candidates should recognize imaging artifacts, utilize non-imaging transducers, and adjust ultrasound console settings for optimal imaging and Doppler recordings. Knowledge of harmonic imaging, principles of contrast agents, and the safe and effective use of saline and echo-enhancing contrast agents is essential. Candidates must also be able to optimize images when using contrast agents to ensure diagnostic quality.
Free ARDMS AE-Adult-Echocardiography Exam Actual Questions
Note: Premium Questions for AE-Adult-Echocardiography were last updated On Jul. 06, 2026 (see below)
Which unit of measurement is used to quantify tricuspid annular plane systolic excursion?
Tricuspid annular plane systolic excursion (TAPSE) is measured as the linear displacement of the tricuspid annulus during systole and is expressed in centimeters (cm). It quantifies right ventricular longitudinal systolic function.
Centimeters per second is a velocity measurement used in tissue Doppler imaging. Milliliters per minute refers to volume flow, and millimeters of mercury measures pressure.
This is standardized in the 'Textbook of Clinical Echocardiography, 6e', Chapter on Right Ventricular Functional Assessment20:320-325Textbook of Clinical Echocardiography.
Based on this video, what is the estimated right atrial pressure in millimeters of mercury (mmHg)?
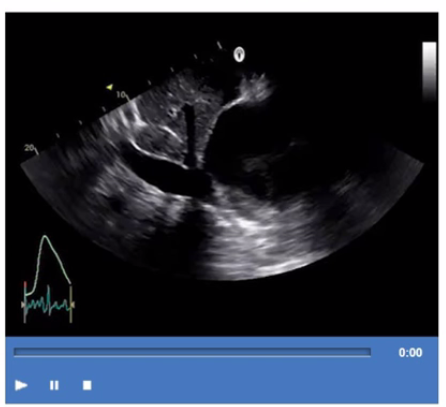
Comprehensive and Detailed Explanation From Exact Extract:
The video shows a subcostal IVC view with measurement of IVC diameter and respiratory collapsibility. The IVC appears dilated (>2.1 cm) with less than 50% collapse on inspiration, suggesting elevated right atrial pressure (RAP).
According to ASE guidelines for noninvasive RAP estimation, an IVC diameter >2.1 cm with <50% collapsibility corresponds to an RAP of approximately 10 mmHg.
Lower RAP values correspond to smaller IVC and greater collapsibility. This is a standard measurement in adult echocardiography practice and ASE chamber quantification guidelines12:ASE Chamber Quantification Guidelinesp.80-8516:Textbook of Clinical Echocardiography, 6ep.115-120.
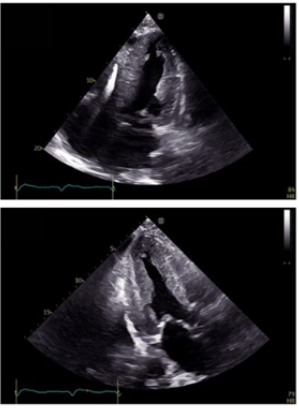
Which diagnosis is most consistent with the findings in these images?
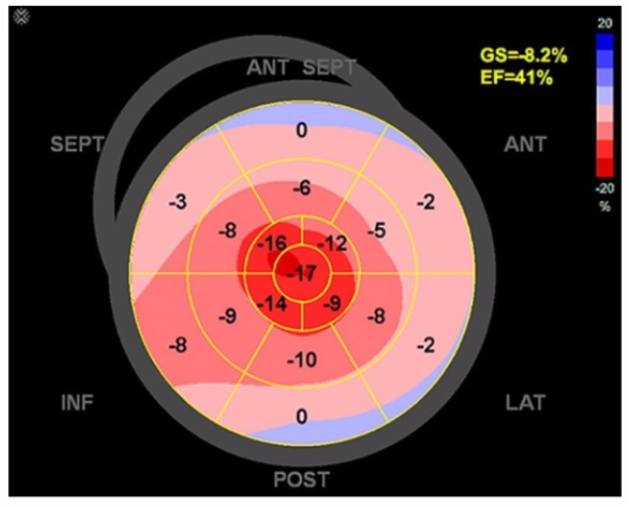
The first image shows a bullseye plot of global longitudinal strain (GLS) with marked reduction in strain values (less negative numbers) most prominently in the apical segments (central red zone), with an overall GLS of -8.2% (normal is about -20%) and a reduced ejection fraction of 41%. This pattern is characteristic of Takotsubo cardiomyopathy, which typically demonstrates regional wall motion abnormalities that predominantly involve the apex and mid segments of the left ventricle with basal sparing.
The 2D echocardiographic images show apical ballooning, a hallmark of Takotsubo cardiomyopathy, where the apex is akinetic or dyskinetic and the basal segments contract normally or hypercontract. Doppler images show findings consistent with impaired ventricular function.
In contrast:
Apical hypertrophic cardiomyopathy (HCM) would show increased wall thickness localized to the apex but not apical ballooning or reduced strain in that typical pattern.
Hypertrophic obstructive cardiomyopathy (HOCM) involves basal septal hypertrophy with outflow obstruction, not apical akinesis or ballooning.
Restrictive cardiomyopathy from amyloidosis involves diffuse infiltration and generally a different strain pattern with more uniform reduction and ''apical sparing'' rather than apical involvement.
This interpretation aligns with the diagnostic criteria and echocardiographic features described in the adult echocardiography literature, including the 'Textbook of Clinical Echocardiography' (Chapter on Cardiomyopathies) and ASE guidelines, which highlight apical ballooning and regional strain abnormalities as diagnostic features of Takotsubo cardiomyopathy16:Cardiomyopathy ChapterTextbook of Clinical Echocardiography, 6e12:ASE Guidelines on Strain Imagingp.130-135.
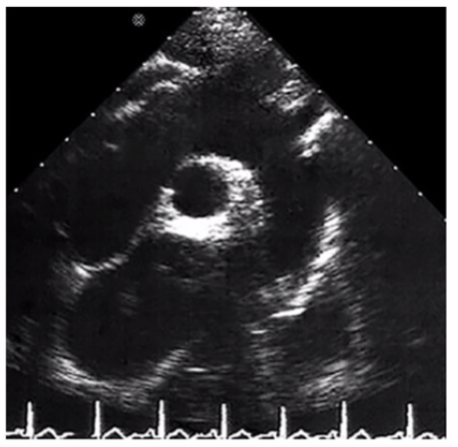
Which finding is shown in this image?
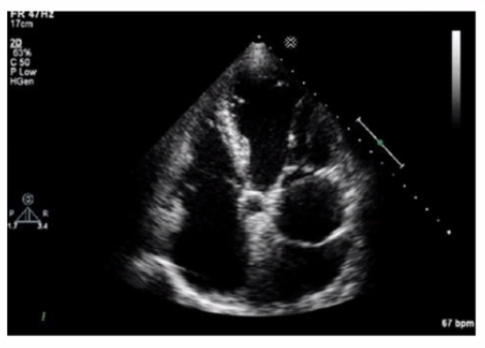
The echocardiographic image shows a mobile, highly echogenic, mesh-like structure within the right atrium consistent with the Chiari network. The Chiari network is an embryologic remnant of the right valve of the sinus venosus, appearing as a fenestrated, reticulated membrane that is usually thin and mobile, found near the orifice of the inferior vena cava or the coronary sinus.
This structure is benign and often an incidental finding but can be confused with thrombus or atrial tumors. Unlike left atrial thrombus, which appears as a more solid, immobile mass often located in the left atrial appendage, the Chiari network is mobile and located in the right atrium. Cor triatriatum is a rare congenital membrane dividing the left atrium into two chambers and appears differently on echocardiography. Artifact refers to non-anatomic echoes which do not persist or move consistently.
Recognition of Chiari network is important to avoid misdiagnosis, and its characteristics are well described in echocardiography literature such as the 'Textbook of Clinical Echocardiography' and ASE imaging guidelines16:Textbook of Clinical Echocardiography, 6ep.400-40212:ASE Guidelines on Cardiac Massesp.150-155.
Identify the right pulmonary artery.
Using your mouse, place the cursor on the appropriate region of the image and then left click the mouse button to indicate your selection.
Which mitral regurgitation jet direction is most consistent with hypertrophic obstructive cardiomyopathy?
Comprehensive and Detailed Explanation From Exact Extract:
In hypertrophic obstructive cardiomyopathy (HOCM), systolic anterior motion (SAM) of the anterior mitral leaflet causes posteriorly directed mitral regurgitation (MR) jets. The abnormal anterior leaflet motion leads to incomplete leaflet coaptation and regurgitant flow directed toward the posterior left atrium.
Anterior jets are seen with posterior leaflet abnormalities. Central jets are seen in functional MR. Medial jets are less common and depend on leaflet pathology.
This jet direction is an important echocardiographic feature distinguishing HOCM-related MR and is outlined in ASE valvular heart disease and cardiomyopathy guidelines12:ASE Valvular Regurgitation Guidelinesp.220-22516:Textbook of Clinical Echocardiography, 6ep.350-355.
- Select Question Types you want
- Set your Desired Pass Percentage
- Allocate Time (Hours : Minutes)
- Create Multiple Practice tests with Limited Questions
- Customer Support
Cynthia Garcia
6 days agoEdward Green
24 days agoStephen Lopez
1 month agoWilliam Hill
2 months agoStephanie Wilson
2 months agoDennis Flores
3 months agoMichael Allen
3 months agoJeffrey Thompson
2 months agoTiffany Parker
2 months agoAmanda White
2 months agoEladia
3 months agoAlesia
4 months agoAnnelle
4 months agoFlo
4 months agoJacki
4 months agoLyla
5 months agoElouise
5 months agoKristel
5 months agoCaren
5 months agoLeonora
6 months agoDorinda
6 months agoCortney
6 months agoArlean
6 months agoNana
7 months agoTanja
7 months agoDierdre
7 months agoShawnda
7 months agoHelga
8 months agoSabina
8 months agoMalissa
8 months agoAlberta
8 months ago